
IBS VA Ratings Explained: Getting the Right % and C&P Exam Tips
Many veterans fight hard to get IBS service connected, only to end up with a 0% rating.
Despite dealing with daily pain, diarrhea, constipation, and constant urgency, many leave their C&P exam feeling like their symptoms were dismissed.
The truth is, once you’re service connected, you’ve already done the hard part.
From there, getting the correct rating usually comes down to clearly showing how often your bowel episodes happen and how your abdominal distress is tied to them.
This guide explains exactly how the VA rates IBS, how to handle a tough C&P examiner, and what to do if you were underrated or denied.
Quick Summary of VA IBS Ratings
- The VA Changed IBS Rating Rules. IBS ratings now focus on measurable frequency and documented abdominal pain tied to bowel movements, often requiring veterans to track and log symptoms.
- The VA Doesn’t Rate IBS on Pain Alone. The VA is not rating how bad your pain feels. They are rating whether abdominal pain occurs during bowel episodes.
- Severe Diarrhea or Constipation Isn’t Enough. These are common IBS symptoms, but they do not qualify by themselves. You must clearly show how they cause abdominal pain during bowel events.
- C&P Examiner Errors Are Common but Fixable. Examiners frequently miss evidence or document symptoms poorly. This can often be corrected through a Higher-Level Review.
- Conflicting Records Lead to Denials. The VA relies heavily on consistency. If your statements change without explanation, it can hurt your credibility and your rating.
How the VA Decides Your IBS Rating
As of May 19, 2024, the VA primarily rates IBS based on how often you have abdominal pain related to bowel movements.
In addition, you must also have at least two of the following: change in stool frequency, change in stool form, altered stool passage mucorrhea, abdominal bloating, or subjective abdominal distension.
The New IBS Rating Criteria (10%, 20%, 30%)
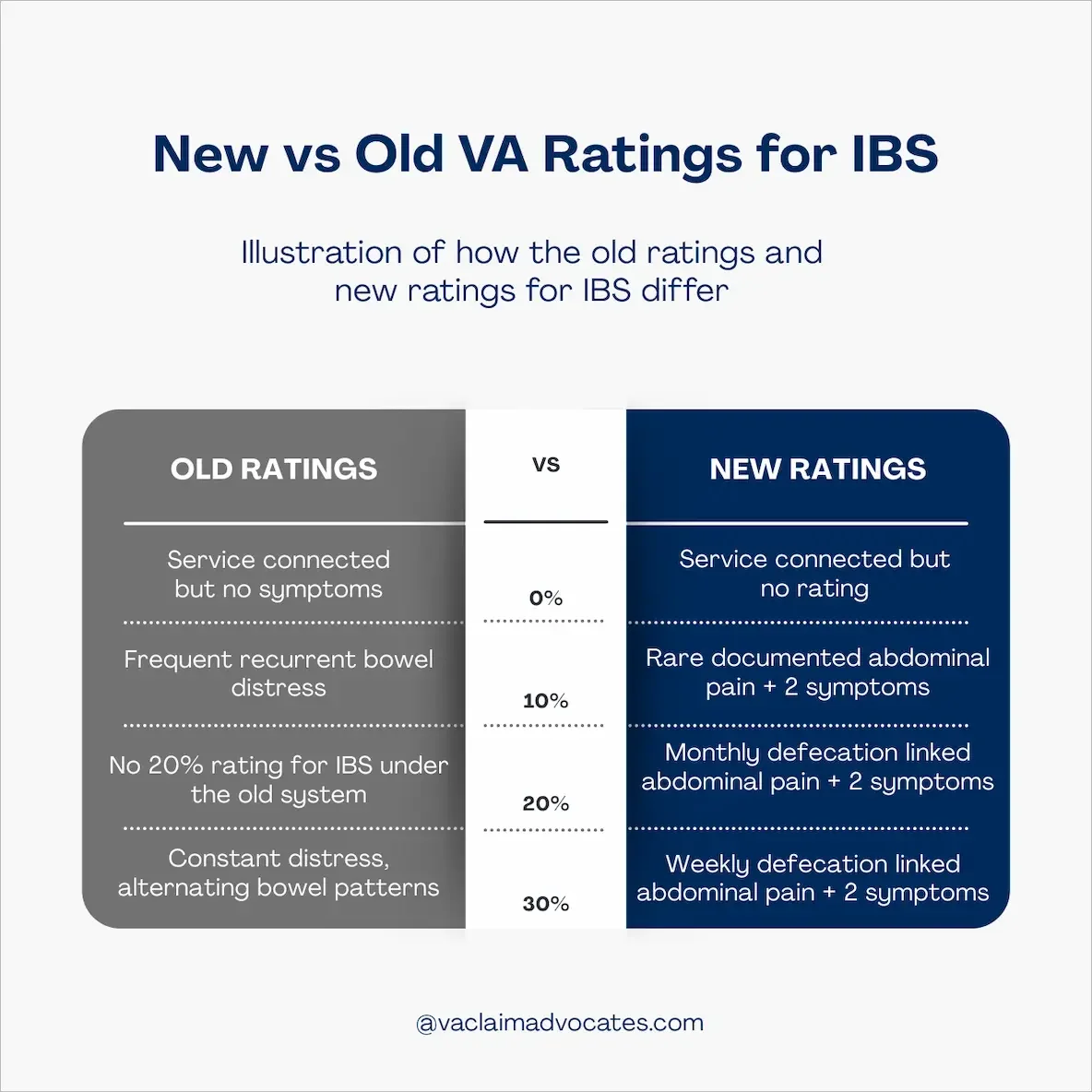
The VA now rates IBS under 38 CFR §4.114, Diagnostic Code 7319 using the following levels:
0% – Symptoms don’t meet the required frequency of abdominal pain tied to bowel movements and/or don’t include at least two qualifying IBS symptoms.
10% – Abdominal pain related to bowel movements at least once in the past three months, plus at least two qualifying symptoms (like stool changes, urgency, bloating, mucus, or distension).
20% – Abdominal pain related to bowel movements at least three days per month in the past three months, plus at least two qualifying symptoms.
30% – Abdominal pain related to bowel movements at least once per week in the past three months, plus at least two qualifying symptoms.
The new rating criteria were built to give veterans more flexibility, since you no longer have to show diarrhea to qualify for a compensable IBS rating.
What the VA Means by “Abdominal Distress”
The VA typically considers abdominal distress to mean physical pain that’s directly connected to bowel issues.
That can include:
Diarrhea
Constipation
Excessive gas
But here’s the key point: the VA does not automatically assume those symptoms equal abdominal distress.
You have to clearly explain and document how those bowel problems actually cause pain or discomfort in your case.
What Actually Qualifies for a 30% IBS Rating
Getting a 30% rating for IBS follows the same structure as the lower ratings. The difference is frequency, not intensity. The VA requires two things:
1. Abdominal pain tied to bowel movements at least once per week
This must occur consistently over the past three months. The VA wants to see a clear pattern, not vague language like “pretty often.”
2. At least two qualifying IBS symptoms
In addition to the weekly abdominal pain, your records must show at least two of the following:
Change in stool frequency
Change in stool form
Altered stool passage, such as urgency or straining
Mucorrhea
Abdominal bloating
Subjective abdominal distension
To reach 30%, you don’t have to prove the pain is worse. You have to prove it happens more often and with more documentation. I will cover more on that later.
Why Many Veterans Get a 0% or Low IBS Rating
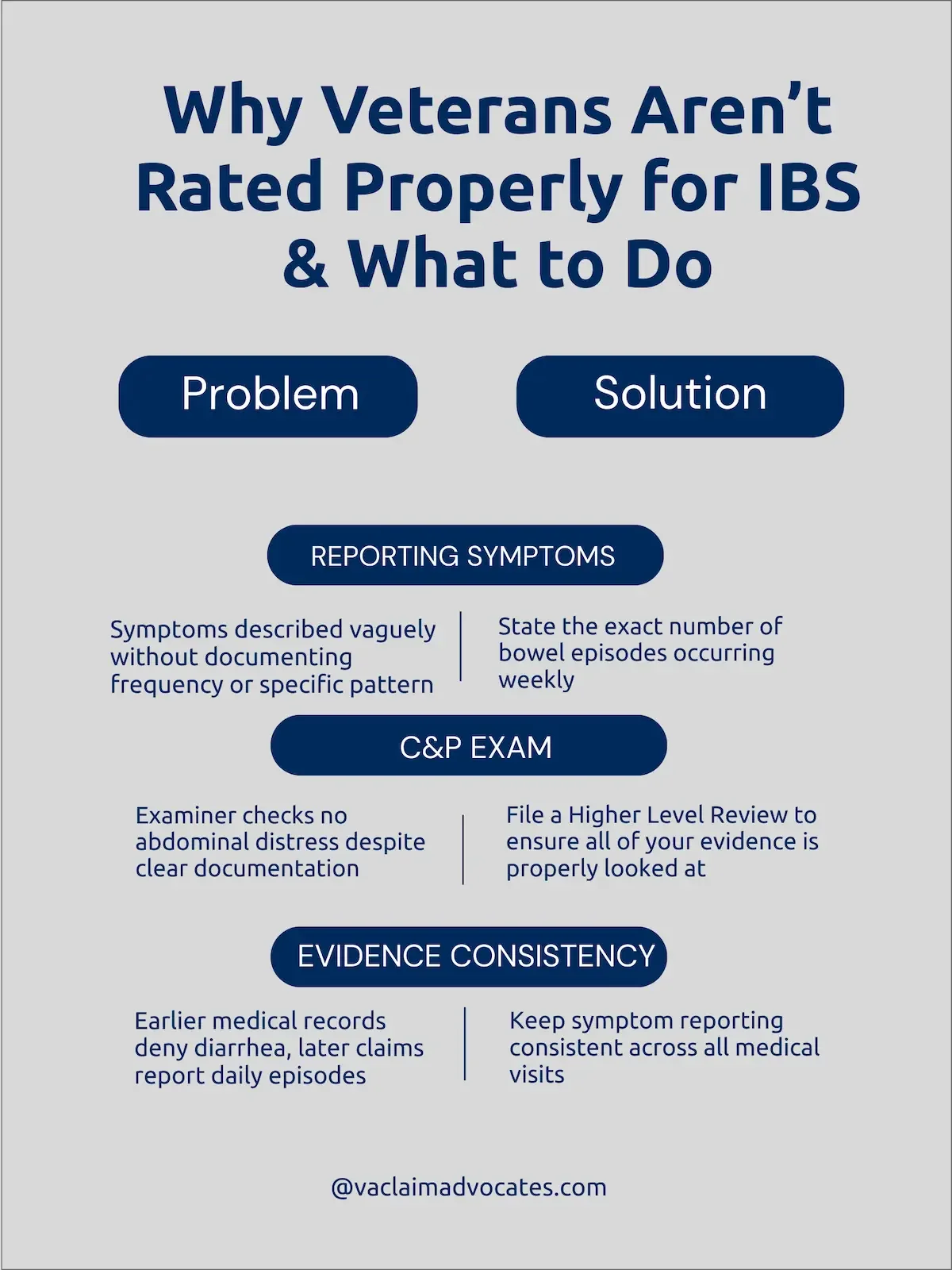
Veterans usually get the wrong IBS rating because they don’t clearly connect their pain to specific bowel episodes, or the C&P examiner fails to write those details down accurately in the exam report.
Not Clearly Connecting Pain to Bowel Episodes
Not reporting your symptoms properly is the fastest way to get denied. Here are a few common mistakes most veterans don’t realize they’re making:
Not tying pain to bowel events – The VA only looks at episodes where abdominal pain is clearly linked to diarrhea or constipation. They don’t care how bad your pain is if you don’t connect it to a bowel episode.
No documented frequency – Telling the examiner how you generally feel isn’t the same as giving a specific number of abdominal pain–related bowel events per week or month. Without numbers, the VA can’t assign a higher rating.
Wording that’s clearly designed for a rating – You should explain how often this happens, but if you say things like “I experience abdominal pain related to defecation at least one day per week during the previous three months,” the VA knows what your doing.
Describe what a typical week actually looks like, use real numbers, explain the daily impact, and avoid legal-sounding rating language.
C&P Examiner Mistakes That Lower Ratings
When the C&P examiner doesn’t report the symptoms you described or doesn’t reference your evidence, it can be maddening.
Common examples include:
“No abdominal distress” box checked – Very common, even when the examiner documents abdominal pain elsewhere in the report.
Failure to review records – Ignoring evidence like prior treatment notes, lay statements, or DBQs.
Not connecting symptoms – Listing diarrhea and pain separately, even though you explained they happen together.
If your examiner made any of these mistakes, the easiest way to correct them is to file a Higher-Level Review.
Inconsistent Medical Records
Many veterans end up with a 0% rating because their records don’t tell a consistent story over time.
Examples include:
Inconsistent reporting – If earlier records say no cramping or diarrhea and you later report both without any explanation, that raises a red flag.
Changing symptom descriptions – Describing symptoms as mild at one visit and severe at another, with no context for what changed.
Exaggerated buddy statements – Family members sometimes overstate the condition in lay statements, which can hurt credibility instead of help it.
The VA understands that IBS can fluctuate. What they’re looking for is whether your overall record makes sense when viewed together.
Best Evidence to Increase Your IBS Rating
To receive the correct IBS rating, your evidence needs to clearly show how often your bowel issues cause abdominal pain.
Keep your records consistent and detailed so the VA sees a clear pattern, not language that sounds crafted for a rating.
Track Your Symptoms the Right Way
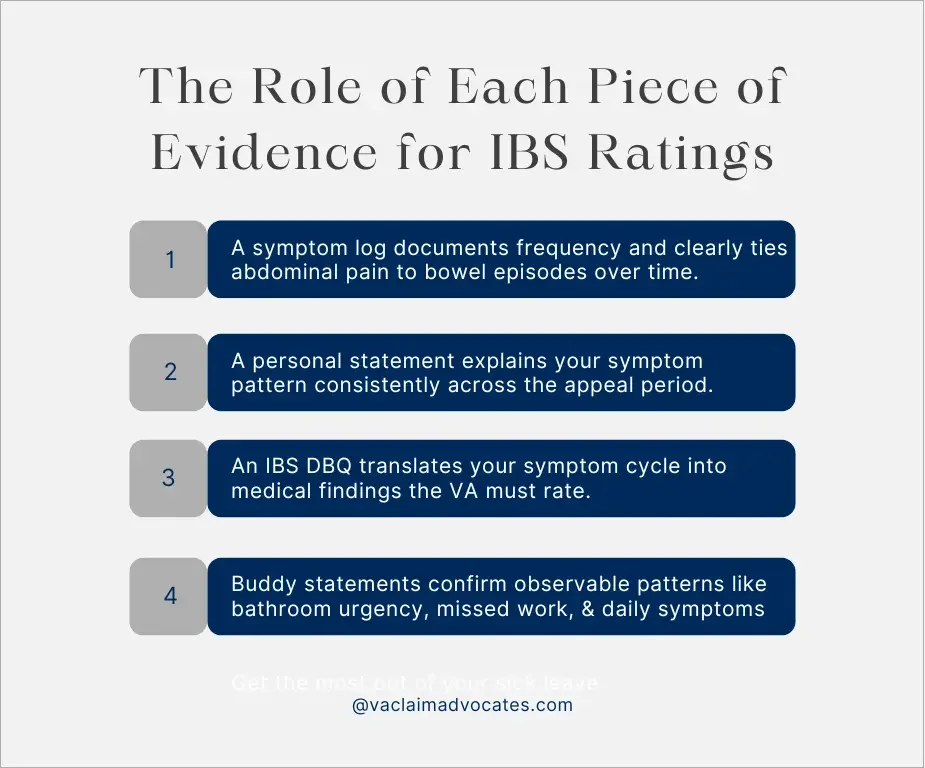
A symptom log shows exactly how your abdominal pain lines up with your bowel movements, which is what the VA actually rates.
Track:
Number of bowel movements or diarrhea episodes per day
Abdominal pain during bowel movements (rate it 1–10)
Other related symptoms
Medication use and whether it helped
The goal isn’t to write pages every day. It’s to make it easy for the VA to see clear patterns over time at a glance.
How to Write a Strong Personal Statement
Your goal in a personal statement is to explain how often your symptoms happen, how severe they are, and how they affect you over time.
Here’s what it should include:
Brief Background: When your IBS symptoms started and how they progressed.
Frequency of Episodes: How often episodes happen using real numbers per day, week, or month. If you don’t define frequency, the VA may assume your symptoms are only occasional.
What a Typical Episode Looks Like: What happens during an episode, including diarrhea or constipation and the abdominal pain tied to it.
Functional Impact Without Medication: How IBS affects your work or daily life, such as frequent bathroom breaks or needing to stay near a restroom. Keep it specific and practical.
When Buddy Statements Help
Buddy statements help because they give the VA confirmation of your symptoms from someone other than you.
While not as strong as a personal statement or DBQ, they show how your IBS affects you from the outside.
Examples:
A spouse explains that you are constantly running to the bathroom.
A coworker confirms you leave meetings multiple times per day.
A friend notices you leave social events early or stay close to restrooms.
Keep buddy statements limited to what the person has directly observed. They should not try to describe your internal pain or give medical opinions.
Using a DBQ to Strengthen Your Claim
An IBS DBQ is one of the strongest pieces of evidence in an IBS claim because a medical professional documents the symptoms that directly impact your rating.
For it to carry real weight, it needs to do the following:
Be internally consistent: Report consistent dates, symptoms, and severity over time.
Match your other records: If you haven’t documented abdominal pain during bowel movements elsewhere, it will look suspicious if the DBQ suddenly does.
Provide explanations: A strong DBQ doesn’t just check boxes. It explains the symptoms and gives detail whenever possible.
A solid DBQ doesn’t guarantee approval at the C&P exam, but it makes it much easier to overturn a denial if you don’t get the right rating the first time.
When IBS Qualifies for Presumptive Service Connection
IBS is not automatically presumptive in every case, but it can qualify if you meet specific Gulf War criteria.
If you qualify, the VA should grant service connection without requiring a traditional nexus opinion.
If you don’t, you’ll need to establish service connection with a medical nexus letter or another way.
IBS Is Usually Considered Presumptive When:
You Have a Formal Diagnosis – You must have a confirmed IBS diagnosis.
Southwest Asia Service – You served in the Gulf War theater, such as Iraq, Kuwait, or Saudi Arabia.
Symptoms Meet at Least a 10 Percent Level – Your symptoms align with at least the 10 percent rating criteria.
Six Month Chronicity – Your symptoms have lasted at least six months.
If the VA denied presumptive service connection because you lacked in-service complaints or treatment records, that is a misapplication of the law, and you should consider filing a Higher-Level Review.
How to Prepare for Your IBS C&P Exam
The best mindset going into a C&P exam for IBS is to assume the examiner hasn’t read your records.
Passing the C&P exam is usually not about whether you’re right, it’s about explaining your symptoms in a way that makes them impossible to miss.
Bring the Right Documents to the Exam
Bringing relevant documents to your exam can help you give clear, accurate answers, and it’s completely appropriate.
Review each document beforehand and highlight the sections that show abdominal pain tied to bowel episodes.
Bring:
Your personal statement
Symptom log
Relevant treatment notes
Your IBS DBQ, if you have one
Having these with you also helps you stay calm and confident, instead of trying to remember everything on the spot.
Reference Your Evidence Naturally
Casually referencing your documented evidence during the exam helps reinforce that you’re consistent and credible.
It shows you’re explaining real, ongoing symptoms, not making things up in the moment.
Examples:
“Over the past three months, I’ve had abdominal pain before or during bowel movements about four days a week.”
“My log shows cramping and urgency at least three times a week, usually right before diarrhea.”
“Most weeks I deal with pain during at least five bowel movements, and I documented that in my treatment notes.”
Just make sure you say it naturally. Reference your records in a conversational way, not in formal, legal-sounding language.
Clearly Link Pain to Bowel Movements
When asked about your symptoms, clearly separate normal bowel movements from the ones that cause abdominal pain.
Examples:
Bad example: “I have diarrhea five times per day.”
Better example: “I have diarrhea about five times per day, and at least four of those episodes come with abdominal cramping and urgency.”
The VA does not assume one symptom automatically causes the other. You need to clearly explain how your bowel episodes and abdominal pain happen together.
Describe Your Symptoms Without Medication
When discussing your symptoms, explain what they look like without medication.
If you only describe how you feel while medicated, the examiner may underestimate how often your symptoms happen and how severe they are.
Be clear about which medications you take and how they help, but focus on what your IBS looks like when you are not taking them.
What the IBS Rule Change Means for You
The new rule change for digestive conditions added more measurable criteria to IBS ratings instead of relying on vague frequency terms.
Most veterans will benefit from this update, but the VA still applies the older criteria if they result in a higher rating.
In addition to these changes, the VA potentially plans to change sleep apnea ratings, PTSD ratings, and tinnitus ratings.
When the New Criteria Help More
If your claim period spans before and after May 19, 2024, the VA must review both the old and new criteria and apply whichever gives you the higher rating.
If your records show near constant abdominal distress with alternating diarrhea and constipation, the old criteria may favor you.
If your evidence clearly shows weekly abdominal pain tied to bowel movements with measurable severity, the new criteria may be stronger.
When You Can Get Separate Ratings for IBS and GERD
Under the updated digestive rules, IBS and GERD don’t get lumped together as easily as they used to.
Before 2024, the VA often combined them under anti-pyramiding because digestive conditions were grouped and treated as overlapping.
The new rules don’t automatically give you two ratings, but they make it easier to separate:
IBS symptoms like diarrhea, urgency, and abdominal pain
GERD symptoms like reflux, regurgitation, and heartburn
If you clearly document them as distinct problems, you have a stronger case for separate ratings.
Bottom Line on Getting the Correct IBS Rating
Getting the right IBS rating can be frustrating, but once your evidence consistently tells the same story, it usually becomes a matter of time.
Most denials happen because of inconsistent documentation or C&P exam errors, not because you don’t qualify.
Stay focused on clear, measurable evidence, and remember that if you win on appeal, you receive back pay for the time you waited.
FAQ
-
The maximum schedular rating for IBS is 30%. However, under the updated digestive rules, IBS and GERD may now be rated separately if their symptoms are distinct, which can increase your overall combined rating.
-
The hardest part is usually proving service connection. Once IBS is service connected, getting the correct rating is straightforward if your evidence clearly documents frequency, abdominal distress, and a consistent symptom pattern.
-
If your rating is lower than expected, review your evidence for gaps. Most low ratings happen because frequency wasn’t clearly documented or abdominal pain wasn’t tied to bowel episodes. Stronger logs and consistent documentation often support an increase.
-
To qualify for 30%, your evidence should consistently show alternating diarrhea and constipation with abdominal distress occurring at least weekly on average. The key is demonstrating a recurring pattern, not isolated symptoms.
-
Sometimes. If your records clearly document frequency and abdominal distress but the examiner failed to record them accurately, an HLR can often correct the error without submitting new evidence.
-
To prove IBS is service connected, you must show a current diagnosis, an in-service event or exposure, and a medical link between the two. This can be direct, presumptive, or secondary to another service-connected condition.
-
Several conditions may develop as a result of IBS, especially when symptoms are chronic and severe. Common secondary conditions include hemorrhoids (from frequent diarrhea or straining), anal fissures, anxiety or depression related to chronic symptoms, and in some cases dehydration or electrolyte imbalance. To claim a secondary condition, you must show a medical link connecting it to your service-connected IBS.